
Dr. Batul Patel (Dermatologist)
Medical Director – The Bombay Skin Clinic
Dr. Batul Patel is an award winning certified dermatologist, honoured as the “Dermatologist of the Year 2023” at the national level by The Economic Times. View profile
What Is Alopecia Areata | Causes of Alopecia Areata | Safety & Side Effects | Treatment Cost in Mumbai
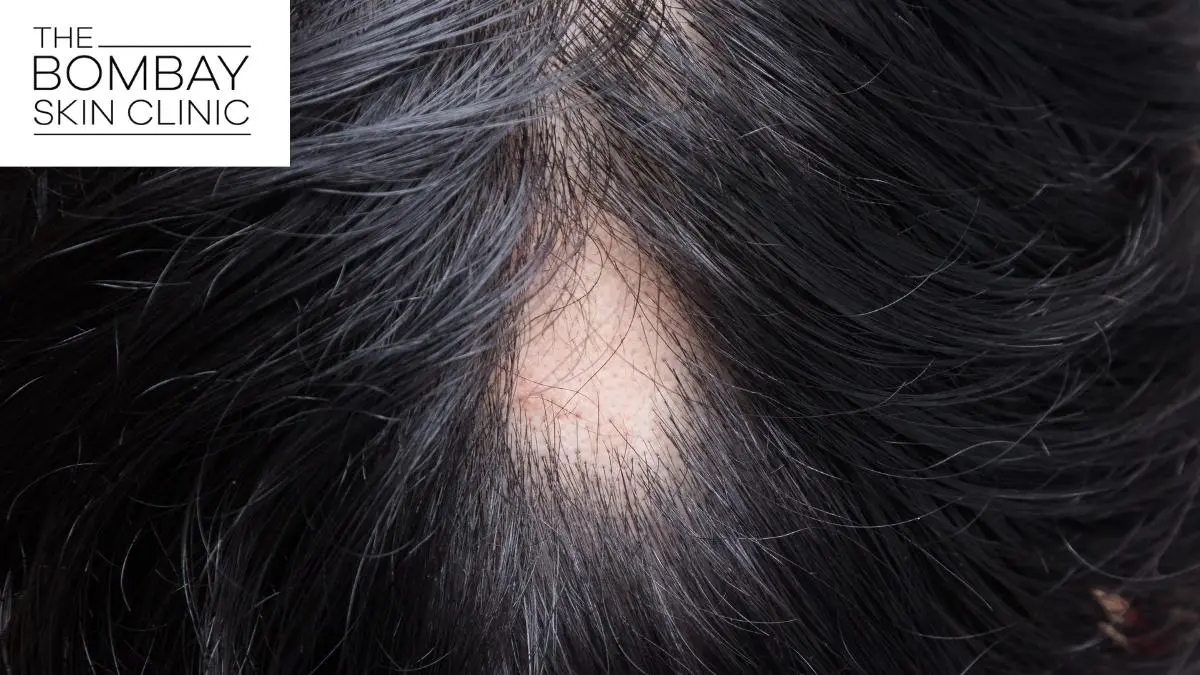
Alopecia areata is a common cause of sudden, patchy hair loss. It is an immune-mediated, non-scarring condition in which the hair follicle is disrupted, but not permanently destroyed in most cases.[1,2]
Many patients first notice one or more smooth bald patches on the scalp, beard, or brows. Because the condition can be unpredictable, early dermatologist assessment matters. At The Bombay Skin Clinic, we approach alopecia areata as a medical hair-loss condition that needs proper diagnosis, realistic counselling, and a plan matched to the extent and activity of the disease. We see patients for hair and scalp concerns across our Mumbai branches in Kemps Corner, Bandra, Andheri, and Chembur.
What is alopecia areata?
Alopecia areata is a form of patchy hair loss that usually appears as round or oval areas of reduced or absent hair. It can affect the scalp, beard, eyebrows, eyelashes, and sometimes other body sites.[1,2]
It is different from everyday hair fall. In everyday shedding, the loss is usually diffuse. In alopecia areata, the loss is often sharply localised. Because the follicles are usually still present, regrowth can happen, but the timeline and pattern vary from person to person.[1,3]
How do you know if your hair loss could be alopecia areata?
Common signs and symptoms
Common clues include:[1,3]
- One or more smooth bald patches on the scalp.
- A sudden patch in the beard, brows, or lashes.
- Localised loss rather than general thinning.
- Short broken hairs at the edge of the patch on examination.
- Nail pitting in a smaller group of patients.
The scalp may look surprisingly normal apart from the missing hair. That is one reason patients may mistake it for a stress-related issue and wait too long before getting it checked.
When to see a dermatologist?
You should book a consultation if you notice a new bald patch, repeated patchy regrowth and relapse, eyebrow or beard thinning in round patches, or hair loss that is starting to spread. A dermatologist should also evaluate you sooner if this is happening in a child, progressing quickly, or affecting confidence significantly.
In Mumbai, patients often assume it is dandruff, stress, or seasonal hair fall. That can delay the correct diagnosis and lead to the wrong over-the-counter products or home remedies.
What causes alopecia areata?
How the immune system affects the hair follicle?
Alopecia areata is understood as an autoimmune or immune-mediated condition. The immune system starts reacting against hair follicles in the active growth phase, which interrupts the normal hair cycle and causes patchy loss.[1,2]
That is why treatment is not only about “stimulating” the scalp. In many patients, the main goal is to reduce the inflammatory activity around the follicle and then support regrowth.
Common triggers, associations and risk factors
The exact cause is not always clear, but recognised associations include personal or family history of autoimmune disease, atopy in some patients, and episodes of stress or illness that may coincide with onset even if they are not the only cause.[1,3,4]
- Past episodes of alopecia areata.
- Family history of patchy hair loss or autoimmune disease.
- Possible association with thyroid disease in some patients.
- Nail changes.
- More extensive or longer-standing disease, which may have a more persistent course.[1,3]
Who is a good candidate for alopecia areata treatment?
Who may benefit from treatment?
Treatment may be worth discussing if you have a recent patch of hair loss, repeated episodes, disease that is enlarging, eyebrow or beard involvement, or patchy loss that is affecting confidence and day-to-day life. Patients with limited patchy disease often do well with focused treatment, while others need closer follow-up because of relapse risk.[3,4]
Who may need additional evaluation before starting?
Some patients need more assessment before treatment begins. That includes children, patients with rapidly spreading disease, those with scalp signs that suggest fungal infection or scarring alopecia, and those with major eyebrow, eyelash, or body-hair involvement. Blood tests may be advised in selected cases, but they are not necessary for every patient.[2,4]
When supportive or adjunct treatments may be considered?
Supportive options may be considered when the goal is to complement the medical plan rather than replace it. Some clinics discuss regenerative procedures such as PRP, but in alopecia areata these are better viewed as adjunctive options in selected patients because the evidence is more mixed than for some other hair conditions.[3]
How is alopecia areata diagnosed?
Clinical scalp examination
Diagnosis begins with a focused history and scalp examination. We assess when the patch started, whether it is enlarging, whether similar episodes happened before, and whether the pattern suggests alopecia areata or another cause of patchy loss.[2,4]
Trichoscopy and patch pattern assessment
Trichoscopy helps a dermatologist look for features that support alopecia areata, such as black dots, yellow dots, broken hairs, and exclamation mark hairs.[1,2]
We also assess the size, number, border, and location of patches because treatment planning changes when the disease is limited, active at the edges, involving brows or beard, or becoming more extensive.
When blood tests or additional work-up may be advised?
Not every patient needs broad testing. But additional work-up may be advised when the history suggests thyroid disease or another associated condition, or when fungal infection or another diagnosis remains possible.[2,4]
How does alopecia areata treatment work?
Calming the immune activity around the follicle
The main medical aim is to reduce the inflammatory or immune activity that is disrupting the follicle. For limited patchy alopecia areata, intralesional corticosteroid treatment is a commonly used option in adults because it targets the affected area directly.[3,5]
Supporting regrowth and scalp recovery
Other parts of the plan may help support regrowth, maintain response, or make the overall routine easier to follow. Depending on the patient, that may include topical options, counselling on camouflage, and structured follow-up.[2,3]
Why treatment plans often need a combination approach?
Alopecia areata can improve, relapse, stay stable, or spread. One patient may need only local treatment and review. Another may need escalation or a combination plan. The right approach depends on extent, age, duration, site involved, rate of progression, and comfort with procedures.[3,4]
What treatment options are used for alopecia areata?
Topical medicines and home-use options
Topical treatments are often considered in milder disease, in patients who prefer a non-injection start, or in children where ease of use matters. They can have a role, but response can be variable and diagnosis still matters before starting them.[3,4]
Intralesional injections for limited patches
For localised patchy alopecia areata in adults, intralesional corticosteroid treatment is a widely used office-based option. It delivers medicine directly into the affected area and may be useful when the number of patches is limited.[3,5]
Oral medicines in selected cases
Oral treatment may be considered in more extensive or rapidly progressive disease, or when the condition is affecting quality of life significantly. These are not first-line for everyone and need closer medical evaluation and monitoring.[3,4]
PRP and regenerative options as supportive treatments
PRP and related regenerative approaches are sometimes discussed in hair-loss clinics. In alopecia areata, they should be framed carefully. They may be considered as adjunctive care in selected patients, but they should not replace proper diagnosis and medical treatment planning.[3]
When light-based or other adjunctive options may be discussed?
Some patients ask about light-based therapies or other supportive procedures. These may occasionally be discussed, but their role in alopecia areata varies and is not the same as a standard first-step medical plan. This is another reason a dermatologist-led consultation matters.
Is alopecia areata treatment safe?
Common side effects
Safety depends on the treatment chosen. With localised intralesional treatment, common issues can include temporary discomfort, local skin thinning if technique or patient selection is not ideal, and the possibility that the patch does not respond fully or relapses later.[3,5]
Contraindications and precautions
Precautions may include active scalp infection, uncertainty about the diagnosis, very extensive disease where another plan may be more appropriate, or patient-specific factors such as pregnancy or concurrent illness. This is why proper medical history is part of the hair consultation, not a formality.[2,4]
- Do not self-start prescription medicines without diagnosis.
- Do not use steroid-based treatment without supervision.
- Seek reassessment if a patch enlarges despite treatment.
- Recheck the plan if new patches appear in other sites.
Special considerations for children, pregnancy and active scalp infection
Children with patchy hair loss need careful diagnosis because fungal infection and other causes can overlap. Pregnancy and breastfeeding require more individual treatment selection. Active scalp infection changes the plan because infection has to be addressed first.[2,4]
What results can you realistically expect and how long do they take?
Early signs of regrowth
Early regrowth can appear as fine, light, or soft hairs within the patch before the area looks fully filled in. The return of density usually takes longer than the first visible sign of change.[3,4]
Usual timelines for visible improvement
Timelines vary. Some patients with limited recent patches may start seeing early change within weeks to a few months. Others take longer, especially if the patch has been present for longer or if new patches continue to appear. Alopecia areata is one of those conditions where realistic timing matters as much as treatment selection.[3,4]
Why relapse or new patches can still happen?
Even when a patch regrows, alopecia areata can relapse because the underlying immune tendency may persist. That is why a good treatment discussion includes both regrowth and recurrence.[1,3]
What affects response to treatment?
Response is influenced by disease extent, duration, site involved, age of onset, nail changes, and whether the disease is limited or becoming more widespread.[1,3]
Alopecia areata vs other causes of patchy hair loss
Alopecia areata vs fungal scalp infection
Alopecia areata usually causes smooth, non-scarring patches. Fungal scalp infection may show scaling, inflammation, broken hairs, or tenderness and is treated very differently.[2,4]
Alopecia areata vs traction-related hair loss
Traction hair loss is linked to hairstyles that pull repeatedly on the hairline or specific areas. The pattern and history are usually different and often point to styling tension rather than immune-driven patchy loss.
Alopecia areata vs telogen effluvium and general hair fall
Telogen effluvium causes diffuse shedding rather than sharply defined patches. Patients usually describe more hair coming out during wash or brushing, not one round area of loss.
Which alopecia areata treatment is better than closely related options?
Injections vs topical treatment
For limited patchy alopecia areata in adults, intralesional treatment is often preferred because it targets the affected area more directly. Topical treatment may still be useful in mild cases, in children, or when injections are not practical.[3,5]
Medical treatment vs PRP or supportive procedures
When alopecia areata is clearly active, diagnosis-led medical treatment usually takes priority. PRP or other supportive procedures may be considered in selected cases, but they are better treated as adjuncts where evidence is mixed.[3]
Alopecia areata treatment vs hair transplant, and when transplant is not the first step
Hair transplant is generally not the first step for active alopecia areata. The issue is not simply lack of hair, it is immune activity around the follicle. A transplant discussion makes sense only in very selected situations after careful diagnosis and stability assessment.
What is the cost of alopecia areata treatment at The Bombay Skin Clinic?
Pricing is indicative and depends on the consultation type, the area involved, whether treatment is localised or more extensive, and whether your plan includes in-clinic procedures or supportive therapies. At The Bombay Skin Clinic, an initial assessment can start from ₹1,000. If your plan includes localised in-clinic treatment or supportive add-ons, the overall cost is higher and is finalised after scalp assessment.
Frequently asked questions about alopecia areata treatment
Can alopecia areata grow back on its own?
It can in some patients, especially with limited patchy disease, but the course is unpredictable. A dermatologist can help decide whether observation is reasonable or whether early treatment is a better option.[1,4]
Is alopecia areata permanent?
Not necessarily. Alopecia areata is a non-scarring form of hair loss, which means regrowth is possible. But it can relapse, and some patients have a more persistent course than others.[1,2]
How many sessions are usually needed?
There is no fixed number that suits everyone. A single recent patch may need a shorter plan than recurrent or more extensive disease. Follow-up is usually based on response and whether new patch activity appears.
Is PRP useful for alopecia areata?
It may be discussed in selected patients as a supportive option, but it should not be positioned as the default answer for everyone with alopecia areata. Diagnosis-led treatment remains the priority.[3]
Can stress cause alopecia areata?
Stress may be associated with the timing of onset in some patients, but it is not the full explanation. Alopecia areata is an immune-mediated condition, so the treatment discussion should not stop at stress alone.[1,2]
When should I book a consultation for bald patches?
You should book a consultation as soon as you notice a new smooth patch, beard or brow patchiness, repeated episodes, or rapid spread. Early assessment helps confirm the diagnosis and reduce delay in correct care.
References
[1] Lepe K, Monrroy A. Alopecia Areata. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK537000/
[2] National Institute for Health and Care Excellence. Alopecia areata. https://cks.nice.org.uk/topics/alopecia-areata/
[3] Sibbald C, Mostaghimi A, Singh S, et al. Alopecia Areata: An Updated Review for 2023. Am J Clin Dermatol. https://pmc.ncbi.nlm.nih.gov/articles/PMC10291119/
[4] National Institute for Health and Care Excellence. Alopecia areata: Diagnosis. https://cks.nice.org.uk/topics/alopecia-areata/diagnosis/diagnosis/
[5] Ibrahim O, Bayoumi A, El-Ghareeb M, et al. Intralesional Steroids for Alopecia Areata. J Cutan Aesthet Surg. https://pmc.ncbi.nlm.nih.gov/articles/PMC3002419/
Dr. Batul Patel (Dermatologist)
Medical Director – The Bombay Skin Clinic
Dr. Batul Patel is an award winning certified dermatologist, honoured as the “Dermatologist of the Year 2023” at the national level by The Economic Times. View profile




